


 720-777-0123
720-777-0123
-
Your Visit
Click to find the locations nearest you
Find locations by region
See all locations -
Research & Innovation

It starts with a Q:
For the latest cutting-edge research, innovative collaborations and remarkable discoveries in child health, read stories from across all our areas of study in Q: Advances and Answers in Pediatric Health.



ACL Graft Options

The anterior cruciate ligament — better known as the ACL — has a very limited healing capacity. Our sports medicine experts take a variety of different approaches for mending torn ACLs, including both surgical and non-surgical options.
Where is the ACL, and what does it do?
The ACL is a type of ligament that is in the knee. Ligaments are tough bands of tissue that connect the ends of bones together.
The ACL is located in the center of the knee joint, where it runs from the backside of the femur (thighbone) to connect to the front of the tibia (shinbone). It has two main functions:
- To prevent the tibia from sliding forward on the femur.
- To prevent the tibia and femur from rotating out of position during various sports movements, such as cutting, twisting and landing activities.
What are my child’s options for ACL treatment?
Your child's orthopedic surgeon will help you navigate the best treatment for your child's ACL tear. They'll consider the percentage of the ACL that is torn, your child's sports and activities, and other factors about your child's injury.
ACL repair or reconstruction surgery is often recommended for kids with ACL tears. But in some cases, your doctor may recommend a different rehabilitation program for your child's injury.
What are the risks and benefits of ACL reconstruction surgery?
When weighing different options for ACL reconstruction surgery, it's important to take both the benefits and risks into account. Below are a few to consider, and your orthopedic surgeon will help you evaluate these options:
- Potential benefits of ACL reconstruction surgery
- Improved knee stability during cutting, twisting and landing activities.
- Lower risk of experiencing additional injuries to the knee, such as meniscus tear(s), cartilage damage and early arthritis.
- Potential risks of ACL reconstruction surgery
- Infection or bleeding.
- Damage to nerves and blood vessels.
- Stiffness.
- Re-tearing (our re-tear rates are less than 4% within 24 months of surgery).
- Growth problems (in children who are still growing).
- Fracture at the harvest site (the part of the body where the graft was taken from).
- Implant failure.
- Need for further surgery.
What type of graft should I choose for ACL surgery: autograft or allograft?
There are two ways that surgeons can reconstruct the ACL using tissue: from either the athlete's own knee, which is called an autograft, or using tissue from a donor, which is called an allograft.
Many researchers, including the ACL study group we participate in with many other hospitals, have studied this question extensively. It's clear that the allograft (with donor tissue) has a much higher failure rate in young athletes. Tissue from the athlete's own body adapts more quickly, predictably and with a much higher rate of success.
Which autograft option is best?
Many factors might affect a young athlete's choice of graft. It usually comes down to a joint decision between the surgeon, the family and the athlete.
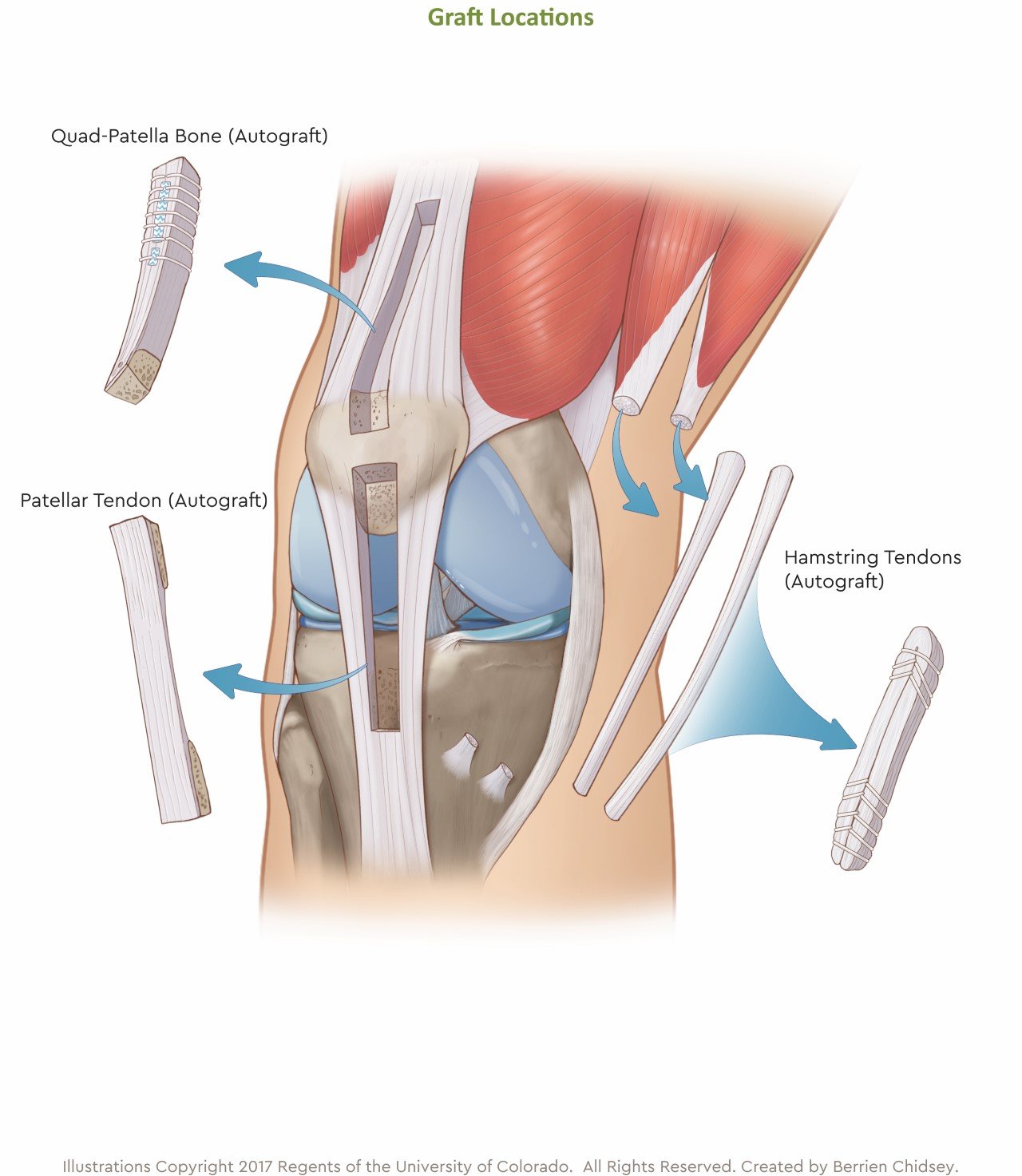
The two most common graft options use either two of the hamstring tendons or a part of the patella (a fancy word for knee) tendon. At Children's Colorado, we also offer a third option, called the quadriceps tendon autograft (also called the quad-tendon graft for short).
Patellar tendon (autograft)
- Strong graft option.
- Longest history of use and long-term follow-up data available.
- More initial graft site soreness.
- Considered by some to be the choice for high-demand, contact athletes.
- Larger incision and more numbness in the front of the knee.
- Higher incidence of long-term pain when kneeling.
- Multiple studies have shown improved long-term results over hamstring grafts, particularly for females.
- Reserved for young athletes who have completed or are close to completing growth (this is not an option for children and adolescents who are still growing due to the location of growth plates in the bones).
Hamstring tendons (autograft)
- Stronger than the patellar tendon graft.
- Causes permanent hamstring weakness.
- Weakened hamstring tendons fail up to 20% of the time in active females.
- Researchers believe that hamstring weakness may be one reason that females are six to eight times more likely to tear their ACLs than males playing the same sport.
- Longer history of use and long-term follow-up data available.
- Slightly more initial graft site soreness and bruising.
- Hamstring muscle left behind has been shown to scar the remaining hamstring muscles and weaken their strength.
- Minimal strength difference compared to other leg.
Quad-tendon (autograft)
- Specifically modified for young athletes.
- This graft posts failure rates lower than all other ACL reconstruction techniques in athletes 10 to 18 years old.
- One of the strongest grafts.
- No permanent weakness.
- Same success rates as patellar tendon.
- Decreased risk of kneeling pain.
- Smaller incision than patellar tendon.
- Can be performed in athletes still growing or done growing.
- Can be considered for high-demand athletes.
- Protects growth plates.
- Eliminates hamstring weakness.
- Re-tear rates of about 2 to 3%, compared to 13 to 23% re-tear rates for hamstring grafts.
What to expect from ACL graft surgery
- The goal of surgery is to return the knee to normal function and stability.
- The surgery will be performed at either the outpatient surgery centers at Children's Hospital Colorado North Campus, Broomfield or Children's Hospital Colorado South Campus, Highlands Ranch outpatient surgery centers.
- Doctors will use general and local anesthesia.
- A new ligament will be made from your own tissue.
- You will likely go home the day of surgery a few hours after the procedure.
What to expect from ACL surgery recovery
- Crutches will be used for 2 to 6 weeks until you gain muscle control and are able to walk without pain in the brace.
- Your physical therapist (PT) or physician will let you know when you are ready to walk without the brace and crutches. Length of time on crutches will depend on associated meniscal or cartilage injury.
- PT is an important component on returning to sport. PT should start 4 to 5 days after surgery. You can expect to be in physical therapy for 9 months, along with home exercises assigned by your physical therapist.
- Performing the PT exercises at home each day is a crucial component of your recovery and return to sports.
- Follow-up visits with your clinician are typically scheduled at 1 to 2 weeks, 6 weeks, 3 months, 6 months, and 1 year after surgery. You will be followed yearly from there until full growth is completed.
- Learn more about the ACL surgery recovery process.
How long will my child be out of sports after ACL surgery?
Your child will be out of sports for a minimum of six to eight months, depending on progress with physical therapy. However, the average is closer to 9 to 10 months.
Why choose Children's Hospital Colorado for your child's ACL graft surgery?
If you or a family member has an ACL injury, our team is here to help. We offer one of the most comprehensive pediatric ACL reconstruction programs in the region, and our experts can answer questions at one of many Children's Colorado locations along the Front Range. We look forward to getting you back in the game.
Learn more about how we diagnose and perform anterior cruciate ligament (ACL) surgery at Children's Colorado.
