720-777-0123
720-777-0123







Key takeaways
-
This retrospective study of patients who ingested button batteries may help inform management with potential risk stratification for development of complications.
-
Battery location is a significant link to severe complications on MRI, with cervical location strongly associated with severe complications.
-
MRI/MR angiography can be a valuable tool to guide clinical management of these patients.
Research background: injuries from button battery ingestion
Lithium button batteries, often found in small electronics and toys, pose a risk for serious injury and death if ingested. An injury is considered mild if only the esophageal mucosa is affected and severe if it extends beyond the wall of the esophagus. Severe injuries include:
- Aortoesophageal fistula (which can lead to death)
- Tracheoesophageal fistula (TEF)
- Mediastinitis
- Spondylodiscitis
- Vocal cord paralysis
Esophageal stricture is a complication that can vary in severity and its presentation is often delayed. Ingestion can cause damage as soon as 15 minutes but can also result in severe and fatal outcomes weeks to months later, even if retrieval occurred within hours of ingestion. There is a need for further study of preventative efforts and more relevant clinical tools to follow these cases and prevent severe outcomes.
The use of radiography in identification, evaluation and follow-up imaging
Lithium button batteries, often found in small electronics and toys, pose a risk for serious injury and death if ingested. An injury is considered mild if only the esophageal mucosa is affected and severe if it extends beyond the wall of the esophagus. Severe injuries include:
- Aortoesophageal fistula (which can lead to death)
- Tracheoesophageal fistula (TEF)
- Mediastinitis
- Spondylodiscitis
- Vocal cord paralysis
Esophageal stricture is a complication that can vary in severity and its presentation is often delayed. Ingestion can cause damage within as soon as 15 minutes but can also result in severe and fatal outcomes weeks to months later, even if retrieval occurred within hours of ingestion. There is a need for further study of preventative efforts and more relevant clinical tools to follow these cases and prevent severe outcomes.
Research methods: a review of MRI findings
The study reviewed the electronic medical records of all patients with button battery ingestions who underwent an MRI at Children’s Colorado between April 2012 and September 2018.
Research results: cervical location of battery strongly linked to severe complications
| Cohort demographics | Median | Range |
|---|---|---|
| Age | 2 | 0.9-17.0 |
| Hours from button battery ingestion to removal, when known | 8 | 2-96 |
| Days in hospital | 15 | 5-65 |
| Days to first MRI | 1 | 0-10 |
| Number of MRIs | 2 | 1-5 |
Of the 23 patients who met the inclusion criteria:
- 16 were male (70%)
- 2 years old median age
- 11 (48%) experienced severe button battery-related complications:
- 11 had esophageal perforations (indicated by air or fluid extending beyond the expected esophageal margin extraesophageal fistulous tract or periesophageal fluid collection)
- 4 had more than one complication:
- 3 had tracheoesophageal fistula (TEF)
- 1 had spondylodiscitis
- 0 had vascular injury
- 1 had vocal cord paralysis diagnosed on bronchoscopy
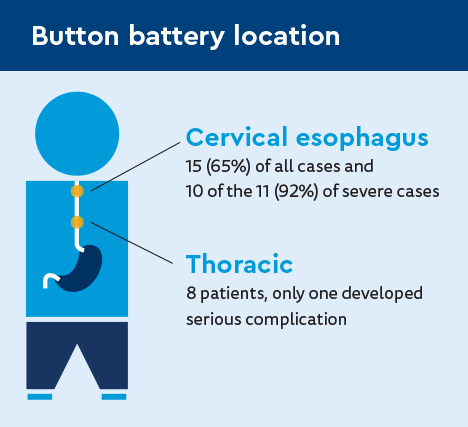
Button battery location
Battery location significantly correlated with severe complications on MRI, with cervical location strongly associated with severe complications.
MRI correlation with clinical findings
- 51 total MRIs/MR angiograms were performed among all patients.
- 19 (83%) had an MRI within three days of button battery removal (one day median).
- 20 had more than one MRI (2.35 average).
- 6.2 days average time between MRIs.
- 8 had more than two MRIs.
- All had extensive edema and enhancement centered at location of battery impaction, extending beyond site of impaction into adjacent soft tissues surrounding the esophagus, trachea and great vessels in the neck and thoracic region.
- All with severe complications had blooming artifact >2 cm.
- Only 2 patients with >2 cm length did not have severe complications.
There was no correlation between esophageal edema/enhancement grading by MRI and severe complications.
Esophageal perforation

There was a moderate correlation with higher esophagram grade and severe complication on MRI.
Of those who had esophagrams:
- 5 found to be normal (correlated with no MRI evidence of esophageal perforation
- 10 found to be abnormal (esophageal irregularity, contained or free leak on esophagram, MRI evidence of esophageal injury)
- 4 had no severe complications
Tracheoesophageal fistula
A probable TEF meant there was obliteration of the fat plane between the trachea and esophagus at the location of button battery ingestion shown on MRI and esophagram. An MRI finding of a normal fat plane between the trachea and esophagus yielded a negative predictive value of 100%, but a positive predictive value of 50% due to blooming artifacts.
Serial MRI examinations
No demonstration of complications after more than one week of battery removal and serial MRI grading produced no significant difference.
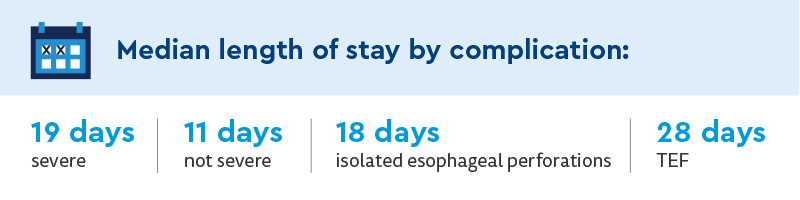
Clinical outcomes
Length of stay significantly longer for patients with severe complications.
Research discussion: MRIs can help identify severity, location and evolution of soft tissue injury and inflammation
Key study findings include:
- Most severe complications occurred, based on imaging, when the battery lodged in the cervical esophagus (92%).
- No significant difference in battery size was seen between patients who did and did not develop severe complication.
- No correlation between the length of time the battery was lodged and the severity of the injury.
- Button battery ingestion has potential for severe, life-threatening hemorrhage from aortoesophageal fistula, which may occur acutely weeks following battery removal even if child appears well.
- The use of MRI to identify severity, location and evolution of soft tissue injury and inflammation following button battery removal at Children’s Colorado helped guide these clinical decisions, avoiding catastrophic hemorrhage.
- A crucial indicator of decreasing risk and safe discharge from inpatient care is when the MRI no longer indicates inflammation in vascular structures.
- Withdrawal of inflammatory changes from vascular structures on MRI is a crucial indicator of decreasing risk and requirement for safe discharge from inpatient care.
MRI/MR angiography provided valuable information, including:
- T1 mDixon GRE sequence was optimal for demonstrating blooming artifact centered at the level of battery lodging.
- Axial and sagittal post-contrast mDixon sequences were also believed to be the most useful in evaluating severe complications, such as TEF, fluid collections and discitis.
- Coronal sequences were the least helpful plane of imaging overall.
Research conclusion: MRIs valuable for managing patients after button battery ingestion and removal
MRI/MR angiography can be a valuable tool to guide clinical management of these patients.
Advantages of MRI over CT:
- Superior soft tissue contrast for vascular and nonvascular structures in the mediastinum
- No ionizing radiation, allowing for better serial imaging
Advantages of MRI for serial evaluation over endoscopy:
- Is noninvasive
- Improved visualization of injury beyond esophagus
- Degree of mediastinal injury in these patients significantly greater than what endoscopy could detect
Additional larger studies and multidisciplinary collaboration would help further define practice guidelines for imaging and management after button battery removal and to study long-term impact of guidelines on outcomes.
Featured Researchers

Lorna Browne, MD
Pediatric radiology specialist
Department of Pediatric Radiology and Imaging
Children's Hospital Colorado
Professor
Radiology-Pediatric Radiology
University of Colorado School of Medicine

Robert Kramer, MD
Co-Medical Director
Digestive Health Institute
Children's Hospital Colorado
Professor
Pediatrics-Gastroenterology, Hepatology and Nutrition
University of Colorado School of Medicine

LaDonna Malone, MD
Pediatric radiology specialist
Department of Pediatric Radiology and Imaging
Children's Hospital Colorado
Assistant professor
Radiology-Pediatric Radiology
University of Colorado School of Medicine

Angie Miller, MD
Radiologist
Pediatric Radiology and Imaging
Children's Hospital Colorado
Associate Professor of Clinical Practice
Radiology-Pediatric Radiology
University of Colorado School of Medicine