


 720-777-0123
720-777-0123







Key takeaways
-
All pediatric patients with anorectal malformations should undergo an early kidney ultrasound to evaluate the renal status and identify obstruction.
-
A bifid scrotum is a common urologic malformation associated with rectobladder neck fistula and may serve as a sign for diagnosis.
-
Rectobladder neck fistula is associated with poor functional prognosis.
-
Close urological follow-up is required.
-
Correct colostomy construction should be addressed.
Research background
Traditional classifications of anorectal malformations in children are categorized as low, intermediate or high. This classification fails to distinguish among different types of anorectal malformations, which may be included in the same category even though they may require different surgical approaches and have different prognoses.
Rectobladder neck fistula is the highest and most complex anorectal malformation in boys. It carries a poor prognosis for bowel control and is the only anorectal malformation that requires open or laparoscopic abdominal repair. Its features should identify it as a separate entity due to anatomic variants in the genitourinary tract.
The lead author of this study, Alberto Peña, MD, of the International Center for Colorectal and Urogenital Care at Children’s Hospital Colorado proposed a more practical classification in a 1995 study titled “Anorectal Malformations” published in Seminars in Pediatric Surgery, which was based on anatomic features of the malformations.
This research study aimed to describe the distinct characteristics of anorectal malformations with rectobladder neck fistula that warrant special attention and to describe associated anatomic variants in the genitourinary tract.
Research methods
All patients treated for rectobladder neck fistula in a database of a tertiary medical center from 1980 to 2011 were included in a review of associated anorectal malformations, type and characteristics of colostomy at birth, sacral ratio, type of main repair surgery and outcome.
There were 111 patients in the study cohort, accounting for 10% of 1,069 pediatric male patients operated on for anorectal malformation during the study period.
Research results
Associated urologic malformations
There were 99 patients (89%) with an anatomic or functional urologic malformation. The most common anatomic malformation was a single kidney, found in 37 patients, and the most common functional disorder was vesicoureteral reflux (VUR) in 40 patients. Forty-two patients with urologic malformations also had non-urologic anomalies.
Without treatment, these abnormalities can lead to significant upper urinary tract complications and lifelong morbidity.
Ectopic verumontanum (VM)
There were 16 patients with a VM located in a higher than normal anatomic position. This group accounted for 40% of children who underwent cystoscopy, which was an unexpected finding.
A potential consequence is infertility, and assisted reproduction techniques should be discussed with patients.
Associated non-urologic malformations
There were 47 patients with non-urologic anomalies; 23 patients of whom had more than one of the associated anomalies. Twenty-nine had cardiac anomalies and 25 had gastrointestinal malformations.
Sacrovertebral anomalies
The most common sacrovertebral anomaly was hemivertebra, occurring in 25 patients. The average sacral ratio (SR) was .59 (calculated from available data on 95 patients).
Colostomy opening
All but one patient underwent colostomy at birth at other institutions. The stoma was located too distally in 20 patients, limiting the bowel for a pull through. Four underwent revision before main repair and 13 needed special treatment maneuvers during the main repair.
Placement of a proper stoma during the newborn period is essential to prevent unnecessary complications.
Surgical approach
The main repair in the 98 patients operated on at the study authors’ institution was posterior sagittal anorectoplasty (PSARP) with laparotomy (80 patients), laparoscopic assisted PSARP (8 patients) and PSARP alone (10 patients).
For surgical repair, the abdominal approach is recommended with a posterior sagittal incision and the laparoscopic approach is particularly indicated.
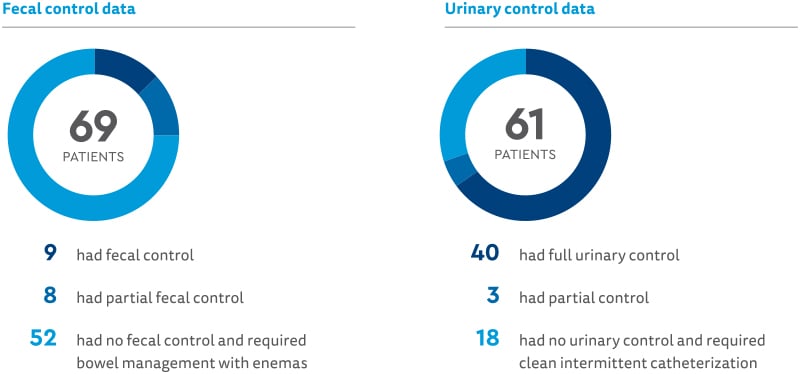
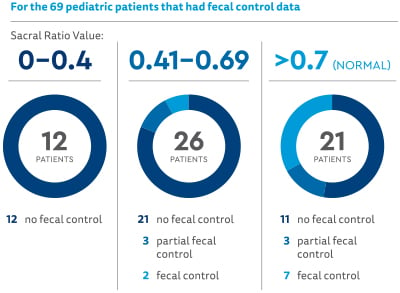
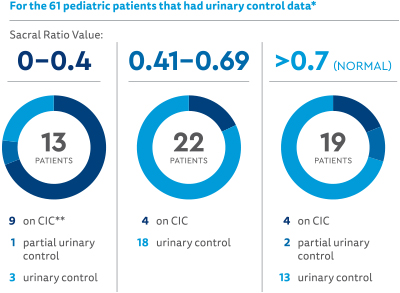
Research functional results
Relationship between sacral ratio (SR) and outcome (SR was divided into three groups):
Featured Researchers
Alberto Peña, MD
Founding Director
International Center for Colorectal and Urogenital Care
Children's Hospital Colorado
Professor emeritus
Surgery


