


 720-777-0123
720-777-0123
-
Your Visit
Click to find the locations nearest you
Find locations by region
See all locations -
Research & Innovation

It starts with a Q:
For the latest cutting-edge research, innovative collaborations and remarkable discoveries in child health, read stories from across all our areas of study in Q: Advances and Answers in Pediatric Health.



Microtia Clinic
Microtia in Children
We see more, treat more and heal more kids than any other hospital in the region.

What is microtia?
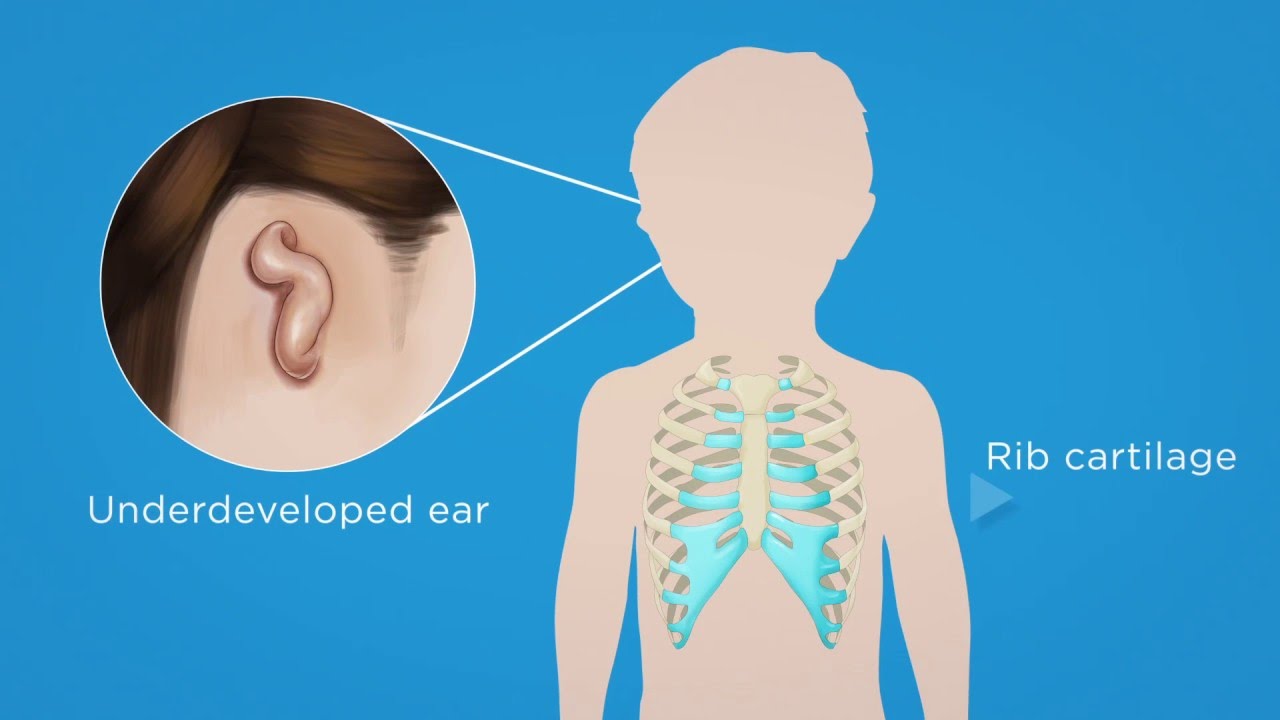
A child with microtia has an ear(s) that isn't fully developed; microtia affects how the outer ear looks. This condition develops before babies are born, during the first four months of a mother's pregnancy.
Ears affected with microtia can be:
- Slightly smaller than normal
- Significantly smaller than normal with differences in parts of the ear
- Absent (anotia)
What is atresia of the ear canal?
A child with atresia is born without an external ear canal. Atresia can be complete where there is no ear opening or there can be a very thin opening of the external ear canal. The level of hearing loss that atresia creates varies depending on the opening.
What is microtia-atresia?
Children with microtia-atresia have both a small or absent outer ear and they are missing an ear canal.
A child with microtia-atresia may have additional health challenges, including syndromes that affect the face like hemifacial microsomia or Oculo-Auriculo-Vertebral (Goldenhar) syndrome.
When an individual has microtia or microtia-atresia and no other developmental conditions, it's called isolated microtia.
Where did the name microtia-atresia come from?
The name can be broken down into "micro," which means small; "otia," which means ear; and "atresia," which means without an opening.
What causes microtia and atresia?
Microtia happens because of a mix of genetic and environmental factors. The exact cause for most patients is not clear. Sometimes, the condition is passed to a child from a parent.
Microtia and atresia has not been linked to anything the mother did or didn't do during pregnancy, except in very rare cases of taking certain prescription drugs. The prescription drugs Isotretinoin (Accutane) and Thalidomide, for example, can cause microtia (and other conditions) when used during early pregnancy. Both drugs are not allowed to be used in women who are pregnant.
Who gets microtia and atresia?
Babies of any ethnicity can get microtia-atresia. However, it's more common in Hispanic and Native American ethnic groups.
Rate of occurrence by ethnicity:
Navajo, Inuit, Andean: 1 in 1,200 live births
Native Americans: 1 in 1,800 live births
Hispanic: 1 in 10,000 live births
Asian: 1 in 10,000 live births
Caucasian: 1 in 20,000 live births
African: 1 in 40,000 live births
What are the signs and symptoms of microtia and atresia?
Microtia can be diagnosed and seen on a 20-week ultrasound. However, it is not routinely evaluated during a normal pregnancy.
Once a baby is born, parents and health care specialists will notice:
- Unusual ear size
- Unusual shape of the outer ear
- A closed or very small ear canal opening
What is the risk of future children having microtia-atresia?
The risk of having a child with microtia-atresia is low. The risk of having more than one child with microtia-atresia is also low unless your ethnicity has a high rate of occurrence, like Native American. However, it is still rare to have parents and children or siblings with microtia-atresia.
What tests are used to diagnose microtia-atresia?
Newborn testing
All newborns with microtia-atresia should receive a diagnostic Auditory Evoked Potentials (AEP or auditory brainstem response/ABR) evaluation within three months of birth. The test can be done as early as any routine newborn hearing screening.
An AEP/ABR evaluation is completed by a Doctor of Audiology (AuD). It is highly recommended that newborns diagnosed with hearing loss find a pediatric audiologist for care. Learn about the Audiology, Speech and Learning Center at Children's Colorado.
Testing for older children
All children should receive a hearing screening when starting public school and then be referred for a diagnostic hearing test. However, hearing loss can be missed in newborns if screening isn't done prior to hospital discharge after birth and/or if follow-up for young children is not recommended by the pediatrician or birth hospital. This can happen if microtia/atresia is only in one ear because hearing loss in one ear is harder to detect.
How do specialists at Children's Colorado make a diagnosis?
In order to diagnose microtia-atresia, your child should see a microtia specialist. When you visit Children's Colorado's Microtia Clinic, a specialist completes an evaluation of the child's ear.
During the evaluation, the specialist:
- Evaluates the outer ear and ear canal (if there is one)
- Tests hearing in both ears, even if the canals are not closed
An otolaryngologist (ear, nose and throat specialist) or a plastic surgeon and an audiologist, who are knowledgeable about microtia, complete the evaluation and provide a diagnosis. Sometimes, the child sees other specialists, such as a speech therapist for a language delay.
Atresia treatment
Atresia is a condition in which a child is born without an ear canal. Atresia can be treated with surgery. Two procedures are available at Children's Colorado:
- A bone anchored hearing aid (commonly known as BAHA)
- An ear canal opening procedure
If the hearing loss is sensorineural (nerve deafness), then hearing aids, preferential seating in the classroom and speech therapy are advised.
Microtia treatment
Microtia is a condition that affects how an ear looks. Depending on the child's and parent's wishes, treatment of the microtia affected ear can be left natural or can be reconstructed.
Reconstruction of the outer ear (ear surgery) can be done with a prosthesis or rib cartilage grafting. Reconstruction usually begins when the child is 6 or 7 years old. Boys with microtia/atresia often wait until they are 8 to 10 years old, which is when the shape of their outer ear becomes important to them.
Microtia-atresia treatment timeline
Below is an example of a timeline of care that is adjusted for each patient's needs.
Birth – 3 years old
- Establish care with an audiologist (hearing specialist)
- Consider a trial with sound amplification and daily use of a BAHA or bone aid
- Early intervention services
- Visit the Microtia Clinic every one to two years
3 – 6 years old
- Hearing (audiology) visits per recommendations by a specialist or as- needed for sound amplification
- Visit the Microtia Clinic annually
6 years old +
- Visit the Microtia Clinic for ear surgery and prosthetic options based on how the ear looks
- Hearing (audiology) care annually or as-needed for sound amplification
What to expect at the Microtia Clinic
The Microtia Clinic is held once a month in the afternoon on a Tuesday at Children's Colorado Anschutz Medical Campus, Aurora. Appointments last 60-90 minutes.
Families meet with the ear, nose and throat specialist, a family consultant and an anaplastologist (who makes prosthetic devices) at the beginning of the visit. They meet with the audiologist as needed for hearing tests, amplification consultations and to schedule future appointments.
Families can stay longer to meet other families and patients, but are not required to do so.
Why choose Children's Colorado to treat your child's microtia and atresia?
Children's Colorado provides patients and their families the unique opportunity to learn treatment and rehabilitative options for microtia and atresia from a team that supports each child with his/her own needs.
Our philosophy allows the individual patient to receive current and accurate information from a surgeon, audiologist, family consultant and anaplastologist. This allows the patient to be confident and feel supported in his/her individual treatment choices for microtia-atresia. Additional supports, such as parent-to-parent, patient-to-patient and psychological and social work resources are available as needed.
Colorado Families for Hands & Voices
Parent-run organization that supports families with children who are deaf or hard of hearing without a bias around communication modes or methodology.
Colorado Hearing Resource Coordinator
Assists families with children birth to 3-years old in obtaining access to funding, community resources, coordination of services and providing expertise about hearing loss.
Colorado School for the Deaf and Blind
Hard of hearing and deaf adult role models who are trained to provide awareness experiences to increase understanding of the needs of a student who is hard of hearing/deaf and to improve this child's sense of identity and self-esteem.
Ear Community
Online support group for individuals with microtia and atresia.
Phonak Guide to Access Planning
Provides information that is important to effectively and independently advocate and be responsible for your communication access supports.
Next steps
-
Would you like to learn more about us?
Learn more about the Microtia Clinic -
Do you have questions about your child’s condition?
720-777-8501
Get to know our pediatric experts.

Steven Hamilton, MD
Otolaryngology


Owen Darr, MD
Otolaryngology, Pediatric Otolaryngology

Brian Herrmann, MD
Otolaryngology, Pediatric Otolaryngology