


 720-777-0123
720-777-0123







Research background: Fecal incontinence is a complication of Hirschsprung disease surgery
Some pediatric patients suffer from fecal incontinence after they undergo surgical repair for Hirschsprung disease. There is little mentioned in the medical literature of this potentially preventable complication, which can negatively affect a patient’s quality of life.
Pediatric researchers in the International Center for Colorectal and Urogenital Care at Children's Hospital Colorado hypothesized that the anal canal can be invaded or completely damaged during the transanal portion of Hirschsprung surgery. This explains the fecal incontinence some children experience.
Researchers developed a specific protocol to evaluate these patients. It is important to differentiate between patients that suffer from constipation and pseudo-incontinence and those with true fecal incontinence.
Research methods: Team reviewed Hirschsprung disease surgery patients during seven-year study period
The research team reviewed pediatric patients who had Hirschsprung disease surgery at other hospitals and presented at their bowel management clinic with fecal incontinence between 2005 and 2012.
Research results: A damaged anal canal was the only significant factor leading to fecal incontinence
The mean age for the Hirschsprung pull-through operation and clinic appointment was similar between the cohorts of patients with damaged anal canals (54 patients) and intact anal canals (49 patients). Soave pull-through was the most common operation in both cohorts.
After correcting multiple variances, the need for re-operation was the only significant factor that increased the odds of having a damaged anal canal. With this information, study authors explored the most influential factors to achieve fecal continence in this population.
Patient demographics were similar among those with and without voluntary bowel movements, including the segment of bowel that involved Hirschsprung disease and type of initial surgery. Researchers discovered that fecal incontinence was associated with re-operation, a patulous anus, a non-dilated colon and a destroyed anal canal.
When analyzed with multivariate analysis, the only significant factor leading to fecal incontinence was a damaged anal canal. Additionally, all Hirschsprung disease surgery patients with a damaged anal canal experienced true fecal incontinence.
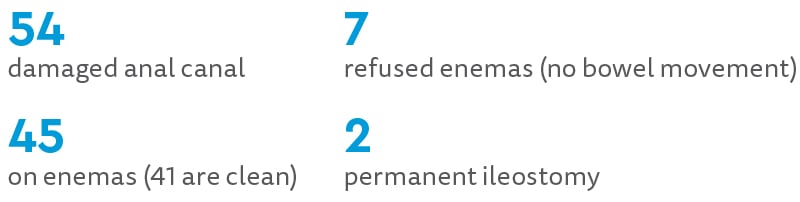
Summary of results: patients with damaged anal canal
Summary of results: patients with intact anal canal

Research discussion: Every effort should be made to preserve the anal canal
Although a technically correct operation for Hirschsprung disease preserves the anal canal to avoid fecal incontinence, there are patients still seeking treatment for this complication.
Most existing literature on Hirschsprung disease surgery in children evaluates long-term outcomes and does not offer a protocol for bowel management for these patients. For those that offer a management protocol, an evaluation of anal canal integrity was not part of the algorithm.
The research team believes their experience is evidence of the importance of preserving the anal canal. There were six patients with an intact anal canal who are totally incontinent, requiring a bowel management program to stay clean. This indicated that there are other factors that contribute to fecal incontinence, perhaps overstretching the anus during Hirschsprung surgery.
It is the team's opinion that every effort should be made by surgeons to preserve the anal canal during operations for Hirschsprung disease.
The researchers recommend using a LoneStar reactor, which provides excellent exposure of the anal canal. The hooks are also advanced in order to fold the anal canal underneath for extra protection.
The surgeon can be very accurate when placing circumferential traction sutures two centimeters above the pectinate line to protect the anal canal. This is where we suspect the sensation resides, a key aspect of bowel control.
Research conclusion: Fecal continence can be avoided in Hirschsprung surgery
Fecal incontinence may occur after surgery for Hirschsprung disease in children and always occurs when the anal canal is damaged. It is severe and probably permanent. This complication may be avoided with a meticulous surgical technique that emphasizes the preservation of the anal canal.


